
When the Scale Stops Moving: Navigating the Anxiety of Weight Maintenance on GLP-1 Medications
There’s a moment almost every patient on GLP-1 medications eventually reaches.
The scale stops going down.
At first, it feels like victory. You’ve lost significant weight. Your clothes fit better. Your energy and labs have improved. Friends and family notice the change.
Then something unexpected happens:
The scale becomes stressful again.
The Dopamine Loop That Breaks
During active weight loss, the scale provides instant feedback and reward:
You step on → the number drops → dopamine hits → motivation stays high.
Once you plateau, that loop shatters.
The number stalls
It fluctuates by a pound or two
What once felt encouraging now feels unpredictable
“Am I regaining?”
This fear is incredibly common—and understandable.
What the Data Actually Shows
In the SURMOUNT-1 extension studies with tirzepatide, patients maintained the majority of their weight loss long-term, but many experienced a modest upward drift after reaching their lowest point (nadir)—most noticeable in follow-up out to about 3 years.
We see a similar pattern after bariatric surgery.
This isn’t failure. It’s biology.
Your body defends a new equilibrium. Your lowest weight on treatment is often your nadir, not your permanent set point.
What This Looks Like Over Time
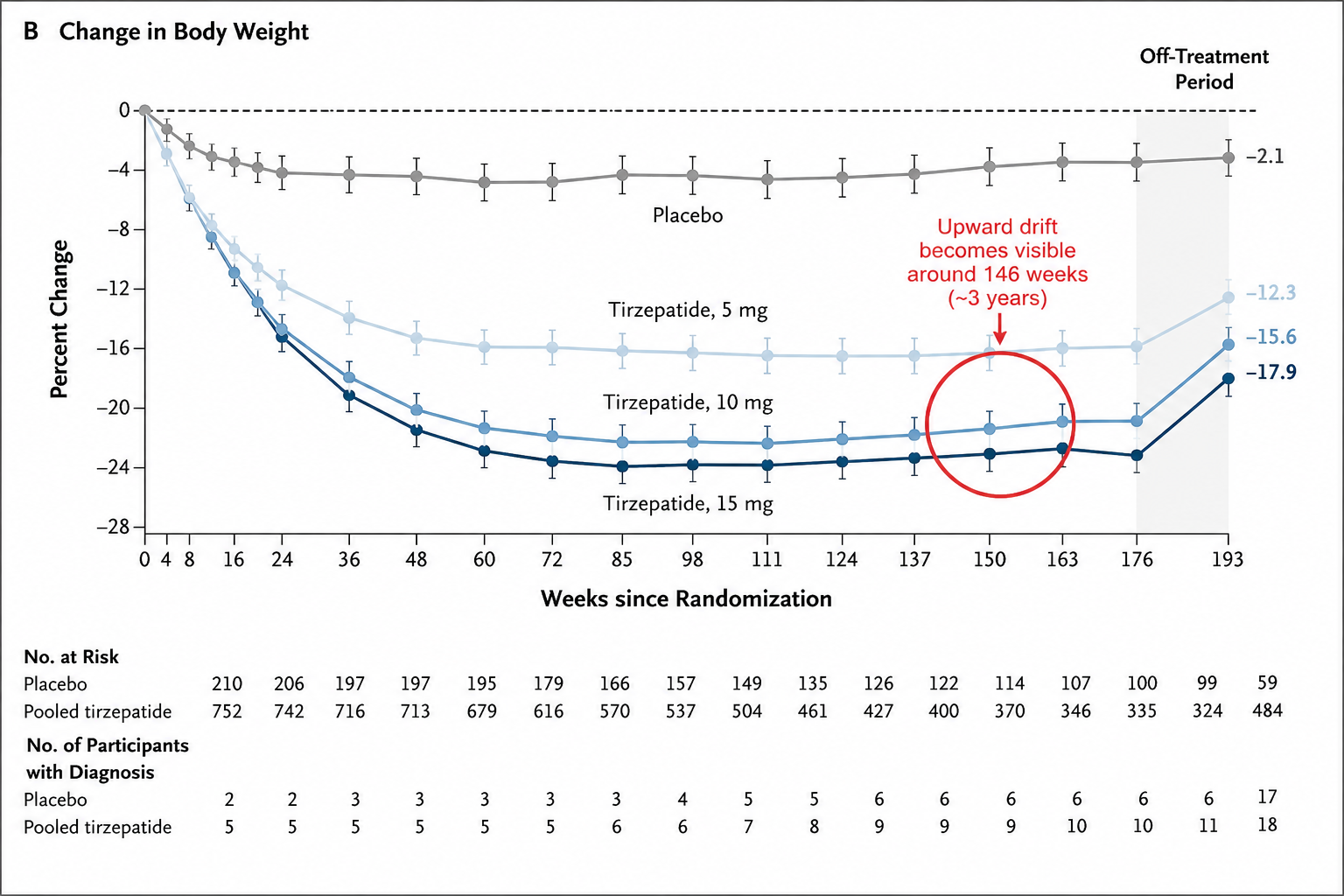
Long-term weight trends with tirzepatide (SURMOUNT-1 extension, ~176 weeks). Weight loss plateaus and is largely maintained over time. Around ~160–165 weeks (~3 years), a small upward drift becomes visible—not a reversal, but a gradual adjustment after reaching the lowest weight (nadir). Most of the initial weight loss is still preserved.
If you look closely, the curve doesn’t just flatten—it subtly turns upward around the 3-year mark (~160–165 weeks).
This is not a sudden regain.
It’s a slow, gradual drift after the nadir.
And most importantly:
The majority of the weight loss is still maintained.
Your Lowest Weight Isn’t Your Permanent Weight
If you lost 25% of your body weight and regain 5%, you’re still down a remarkable 20%.
That’s life-changing success—not setback.
Most People Don’t Recognize Their Nadir When They’re There
You rarely step on the scale thinking, “This is probably as low as it gets.”
More often it’s: “Maybe just a few more pounds.”
So when progress slows—or reverses slightly—it feels like something has gone wrong.
In reality, you’ve likely reached a weight your body can realistically sustain long-term.
Most people don’t recognize their lowest weight when they’re there—they only recognize it after it’s gone.
Normal vs. Not Normal: A Quick Guide
What’s Normal in Maintenance
Plateaus lasting weeks
Daily/weekly fluctuations of ±2–5 lbs
Modest upward drift over months
Natural appetite variability
What Warrants Attention
Consistent upward trend over multiple weeks
Rapid return of intense hunger or food noise
Weight moving meaningfully outside your maintenance range
A Practical Maintenance Framework
Stop reacting emotionally to the scale. Build a simple system instead.
Step 1: Structured Weekly Check-In
One consistent weigh-in per week (same day, same conditions).
Track two additional signals:
Energy: How many days did I feel good energy?
Appetite: Is hunger or food noise creeping back?
These often change before the scale does.
Step 2: Define Your Maintenance Range
Aim to stay within ±3–5% of your lowest achieved weight.
This is your new normal—not a single number.
Step 3: Threshold-Based Action (No Panic)
+2 lbs: Normal noise → do nothing
+5 lbs: Monitor habits, sleep, stress, appetite
+8–10 lbs: Time to adjust your plan
A Simpler Way to Think About Maintenance
During weight loss, the goal is clear: the number goes down.
During maintenance, the goal is different.
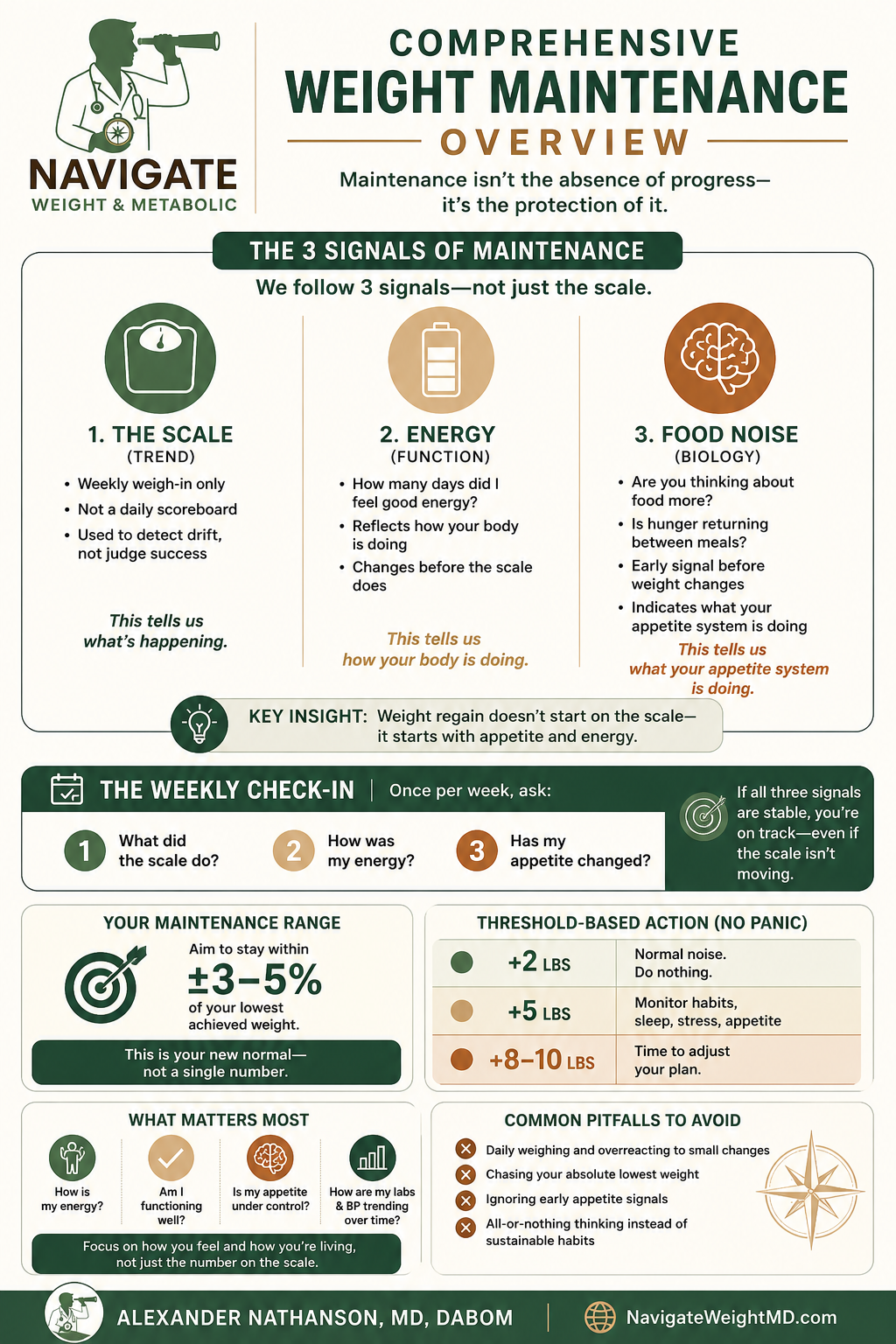
Instead of chasing a number, we follow three signals:
The scale → Are you staying within your range?
Energy → Do you feel good most days?
Food noise → Is your appetite still under control?
Weight is just one piece of the picture.
Your body often tells you what’s changing before the scale does.
A simple weekly check-in is enough:
What did the scale do?
How was my energy?
Has my appetite changed?
This creates a comprehensive weight maintenance overview without overcomplicating things.
If all three are stable, you’re on track—even if the scale isn’t moving.
Real-World Flexibility Beats Trial Rigidity
Clinical trials use fixed doses. Real life allows nuance.
I rarely rush patients to the highest dose. Keeping some “room to move” preserves options for later adjustments.
Options for Dose Adjustment
Extending Injection Intervals
Some patients try spacing injections to every 10–14 days.
This works for some but not for others.
Treat it as a trial.
If hunger increases or weight trends upward: → return to your prior schedule
Transitioning to Oral GLP-1 Therapy
Some patients consider switching to oral GLP-1 options.
This can be more convenient—but generally less potent than injectable therapies.
Some patients maintain but others experience modest weight regain
You’re trading potency for convenience.
Common Maintenance Pitfalls to Avoid
Daily weighing
Reacting to small fluctuations
Chasing your lowest weight indefinitely
Ignoring early appetite signals
All-or-nothing thinking instead of sustainable habits
The Goal Shifts: From Loss to Protection
More weight loss isn’t always better.
At a certain point, the priority becomes protecting what you’ve achieved.
Ask yourself:
How is my energy?
Am I functioning well?
How are my labs and blood pressure over time?
Why Maintenance Feels Harder Than Loss
Your biology adapts.
Metabolism slows
Appetite signals strengthen
Energy expenditure decreases
GLP-1 medications help—but they don’t eliminate biology.
The Exciting Future
We’re still early.
Emerging therapies, including amylin-based treatments, may further improve long-term outcomes.
Final Thought
Weight maintenance on GLP-1s can feel fragile.
But it’s not.
It’s simply a different phase—one that requires a shift from pursuit to stewardship.
The hardest part isn’t losing the weight.
It’s learning to live without the constant reward of seeing it drop.
Maintenance isn’t the end of progress. It is the progress.