
The New Barrier to GLP-1 Care: Insurance “Sludge”
If you’ve tried to access a GLP-1 medication for weight management recently, you’ve probably run into obstacles.
Some of these are familiar:
Prior authorization headaches
High deductibles
Prohibitive copays
But there’s a newer tactic emerging—one that’s less visible, more confusing, and arguably more insidious.
It’s what behavioral economists call “sludge.”
What is “Sludge”?
“Sludge” refers to excessive or unjustified friction in systems that makes it harder for people to access benefits they’re entitled to.
Think:
Unnecessary paperwork
Hidden steps
Delays that serve no clinical purpose
Requirements that look helpful—but function as barriers
Sludge is not accidental. It is often designed.
The Rise of “Compliance Programs”
Insurance companies and pharmacy benefit managers (PBMs) are now adding a new layer of sludge: so-called “compliance programs” (sometimes labeled “utilization management” or “adherence programs”).
Here’s how they typically work:
Patients must enroll in a third-party platform
Complete trainings or modules
Regularly upload weights or health data
Maintain ongoing “engagement” to remain eligible
If a patient is not “in compliance”?
👉 Their medication claim is denied at the pharmacy.
Let’s Be Clear: This Is Not Medical Care
Despite the language used—“support,” “wellness,” “engagement”—there is:
No meaningful therapeutic benefit to these programs.
They:
Do not replace clinical care
Do not improve outcomes in a meaningful way
Do not individualize treatment
What they do accomplish is this:
👉 They insert friction between doctor and patient.
A Real Example: NYC Public Employees
Let’s take a concrete case.
At the end of 2024 New York City made headlines when it cut off coverage for GLP-1 medications for weight loss for thousands of public employees
Many patients—and physicians—assumed that was the end of the story.
But something changed.
With the rollout of a new plan (EmblemHealth / United PPO), coverage appears to have quietly returned.
Except now, it’s buried under sludge.
And most NYC employees likely don’t realize the benefit may still exist.
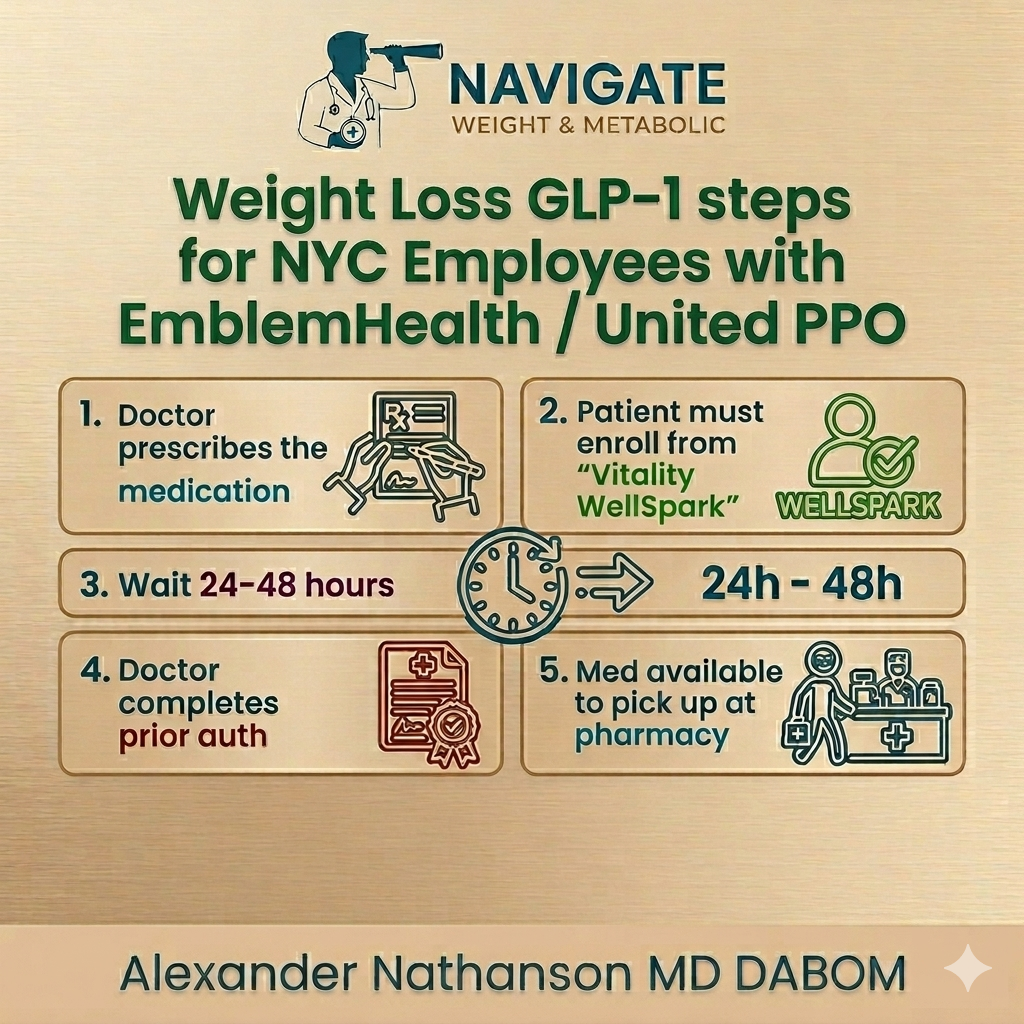
The Actual Workflow
Here’s what patients must now navigate:
Doctor prescribes the medication
Patient must enroll in a program (e.g., “Vitality WellSpark”)
Wait 24–48 hours
Doctor completes prior authorization
Pharmacy claim finally goes through
And that’s just the beginning.
Once on treatment, patients must:
Complete ongoing modules
Submit regular weigh-ins
Maintain “compliance”
Or risk:
👉 Sudden loss of access to their medication
What Makes This Worse
Two major issues make this especially problematic:
1. It’s Not Clearly Communicated
Patients are not told:
That coverage exists
That enrollment is required
How to complete the process
This creates a system where:
👉 People give up before they even start
2. It Undermines the Benefit Itself
Patients and the city are paying into a benefit that:
Many don’t know exists
Many cannot access
Many lose access mid-treatment
That is the definition of ineffective coverage.
Why This Matters Clinically
GLP-1 medications are not just about weight loss.
They have well-established benefits for:
Cardiovascular risk reduction
Fatty liver disease
Obstructive sleep apnea
Emerging and investigational benefits in areas like dementia, cancer, and addiction
These are long-term therapies.
They only work if:
Patients can start them
Patients can stay on them
👉 Sludge directly interferes with both.
The Real Incentive
Let’s be honest about the incentives here.
These programs:
Reduce utilization
Create drop-off points
Shift burden onto patients
Meanwhile, direct manufacturer cash pricing for GLP-1s is gradually falling.
If that trend continues:
👉 Patients may increasingly bypass insurance altogether
The Clinical Reality
Even for experienced physicians, this process is difficult to navigate.
Now consider the standard clinic visit:
5–10 minutes
Multiple competing priorities
No administrative support
It is simply not feasible to:
Explain these programs
Troubleshoot enrollment
Monitor compliance logistics
A Better Model of Care
This is where care models matter.
Patients seeking effective obesity treatment increasingly benefit from:
Longer visits
Direct physician access
Administrative support for medication access
In other words:
👉 Care models designed around the patient—not the insurance workflow
Practices built on this model—such as Navigate Weight & Metabolic—are specifically structured to help patients navigate these barriers, maintain continuity of care, and create a sustainable plan when insurance systems fall short.
A Call to NYC Leadership
New York City leadership should take a close look at what’s happening.
If a benefit exists, patients deserve:
Clear communication
Transparent requirements
Reasonable access
A benefit that is technically present—but practically inaccessible—is not a real benefit.
Bottom Line
Insurance companies are not just denying access outright anymore.
They are doing something more subtle:
👉 They are making access so difficult that patients give up.
That is not a coverage decision.
It’s a behavioral one.
That is sludge.
And in the context of obesity care—where treatment requires consistency and continuity—it is not just inefficient.
It is harmful.