
A Practical Guide to GLP-1 Prior Authorizations (2026)
A New York–Focused Reference for Clinicians
Download PDF here
One of the most frequent questions I get from colleagues is about prior authorizations for GLP-1 medications.
It is also one of the most frustrating aspects of practicing obesity medicine. I spend many hours each week navigating prior authorizations. Many patients are eligible for these medications through their insurance plans but are denied simply because the prior authorization was not completed correctly.
The goal of this guide is to simplify the process.
Some of the details below may be specific to my home state of New York, but many of the principles apply nationally.
This post is primarily written for healthcare providers, but if any well-informed patients believe they qualify for treatment and were denied, feel free to share this information with your medical provider.
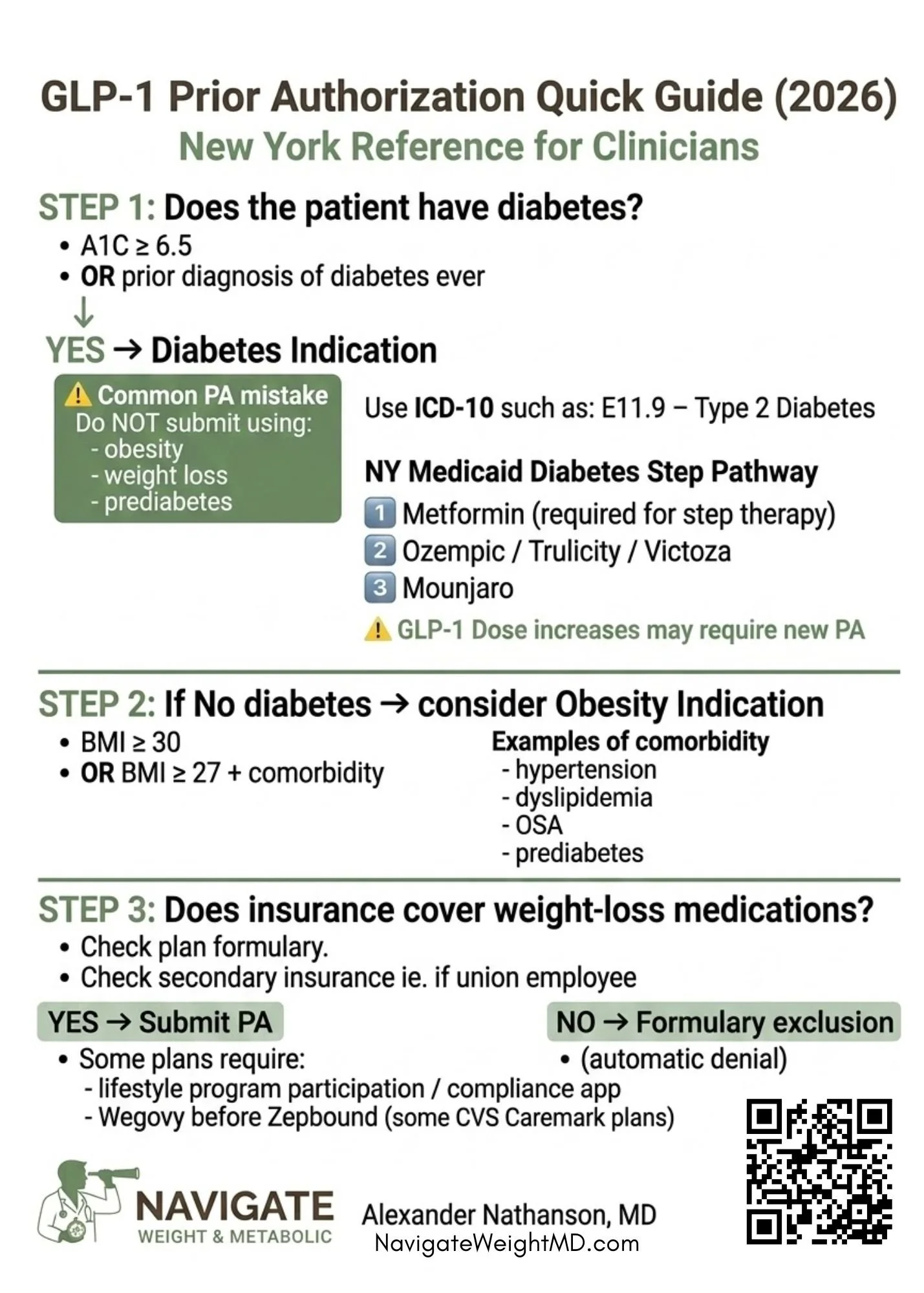
Step 1: Determine Whether the Patient Has Diabetes
The first and most important question is whether the patient has diabetes or has ever had diabetes.
Diabetes is defined as:
Hemoglobin A1C ≥ 6.5%, or
A documented history of diabetes at any time in the past.
The key question is whether the patient has ever met diagnostic criteria for diabetes, even if their A1C has since improved.
For example:
If a patient previously had an A1C ≥6.5 and now has an A1C of 6.0 on treatment, they still qualify for the diabetes indication.
Submitting the prior authorization under obesity instead of diabetes is one of the most common causes of denial.
Important Prior Authorization Tip
The prior authorization must include a diabetes diagnosis code.
Example:
E11.9 – Type 2 Diabetes Mellitus without complications
Do not submit the prior authorization using:
obesity
weight loss
prediabetes
Insurance plans may also require laboratory documentation confirming diabetes.
GLP-1 Coverage for Diabetes
Most Commercial Insurance Plans and Medicare
Commonly covered GLP-1 medications include:
Ozempic
Mounjaro
Trulicity
Victoza
Rybelsus
Some plans require step therapy, ie. trial of Metformin before approval.
New York State Medicaid
For patients with diabetes on NY Medicaid:
Step therapy is required.
Typical sequence:
Metformin
GLP-1 therapy
Commonly approved medications include:
Ozempic
Trulicity
Victoza
Mounjaro is typically approved as third-line therapy.
In New York Medicaid, dose escalation may require a new prior authorization, even when the medication was previously approved.
Step 2: Obesity Without Diabetes
If the patient does not have diabetes, the medication must be prescribed under the obesity indication.
Typical criteria include:
BMI ≥30, or
BMI ≥27 with a weight-related comorbidity
ICD10 code: E66.3 or E66.9
Examples of comorbidities include:
Hypertension
Dyslipidemia
Obstructive sleep apnea
Prediabetes
FDA-Approved Medications for Weight Management
Current GLP-1 options include:
Wegovy
Zepbound
Saxenda (rarely used now)
Commercial Insurance Coverage
For most commercial insurance plans, coverage for obesity medications is binary.
The most important factor is whether the insurance plan includes weight-management medications on the formulary.
If Weight-Management Drugs Are Covered
The patient must meet prior authorization criteria, typically including:
BMI documentation
comorbidities
weight history
If Weight-Management Drugs Are Excluded
The claim will typically be denied automatically.
Unfortunately, these plans often provide no option for appeal, because the medication category itself is excluded.
Formulary Preferences
Some CVS Caremark plans prefer Wegovy over Zepbound.
In these plans:
Wegovy must usually be tried first
Zepbound may be approved after failure or intolerance.
Compliance Programs
Some insurers require participation in a lifestyle or coaching program before approving medication, ie. Wellspark for EmblemHealth plans
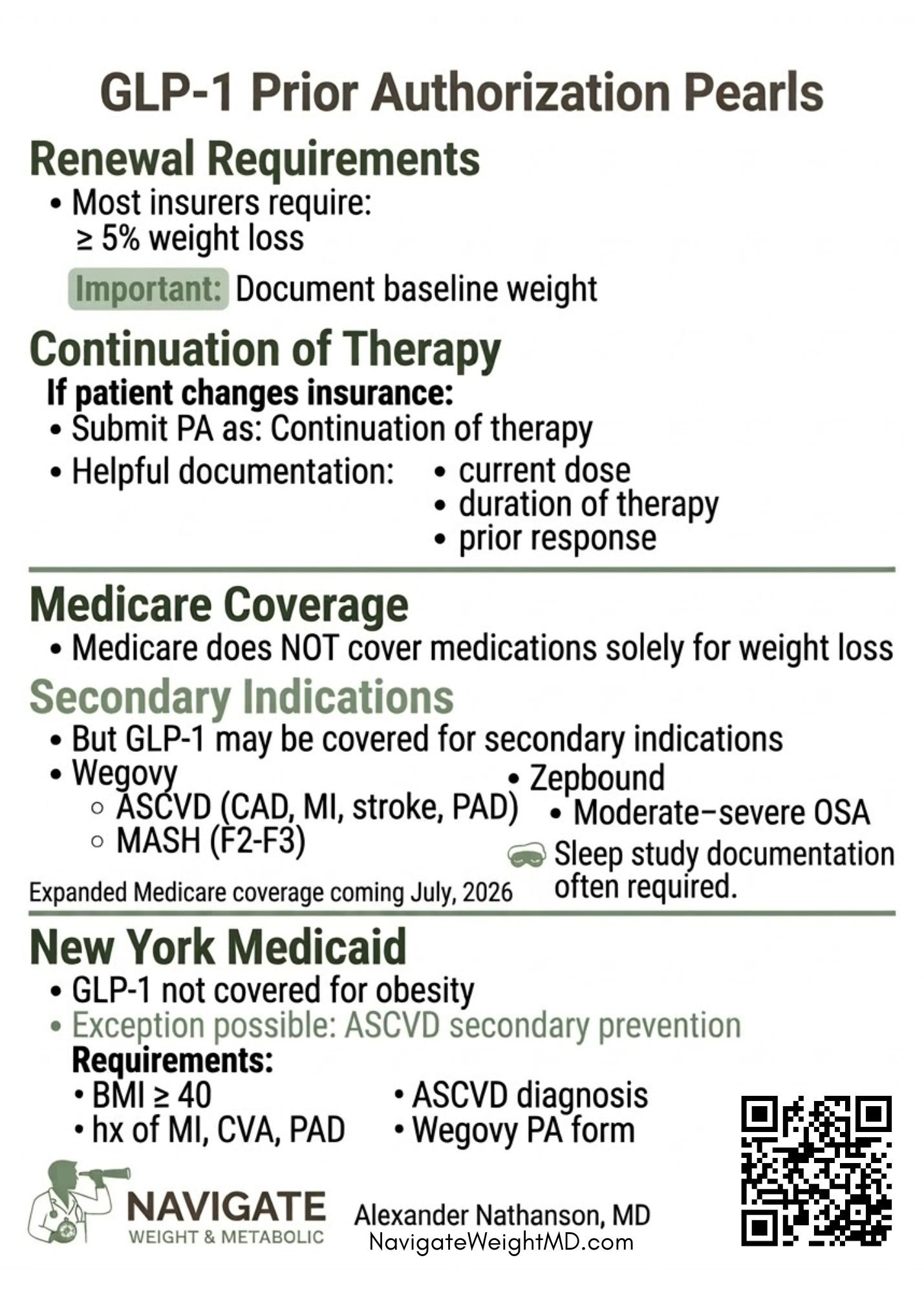
Renewal Requirements
Most insurance plans require documentation of clinical response for continued coverage.
Typical requirement:
At least 5% weight loss from baseline weight.
It is important to document baseline weight at the time the medication is started, as insurers often compare renewal weight to the original starting weight.
Failure to document baseline weight can lead to renewal denials.
Continuation of Therapy
If a patient is already taking a GLP-1 medication but changes insurance plans, the prior authorization can often be submitted as:
Continuation of therapy
Helpful documentation may include:
current medication and dose
duration of therapy
prior weight or A1C response
In some cases, continuation of therapy documentation may help bypass step therapy requirements.
Patients With Multiple Insurance Plans
Some patients have secondary insurance coverage, particularly those with union-based plans.
Example scenario:
Primary insurance denies coverage
Secondary union insurance may cover the medication
It is worth verifying all active insurance plans before concluding that a medication is not covered.
Medicare Coverage Limitations
Medicare does not cover medications used solely for weight loss. This written into Medicare law.
However, GLP-1 medications may still be covered for secondary medical indications.
The qualifying diagnosis must be clearly documented on the prior authorization form.
Secondary Indications Covered by Medicare
Wegovy — Cardiovascular Risk Reduction
Wegovy is approved for secondary prevention of cardiovascular disease in patients with obesity.
Examples include:
Coronary artery disease (CAD)
History of myocardial infarction
Prior stroke
Peripheral artery disease (PAD)
Documentation is usually required.
Wegovy — Metabolic Dysfunction–Associated Steatohepatitis (MASH)
Coverage may be possible for patients with:
Moderate to advanced fibrosis (F2–F3)
Supporting documentation may be required.
Zepbound — Obstructive Sleep Apnea
Zepbound is FDA-approved for treatment of moderate to severe obstructive sleep apnea.
Insurance companies often require:
sleep study results
documentation of severity
Expanded Medicare coverage coming July, 2026. Stay tuned for more details
New York Medicaid and Weight-Loss Medications
In New York State, Medicaid does not currently cover GLP-1 medications for weight management.
Essential Plan
Some patients qualify for the New York Essential Plan, a low-income insurance program separate from Medicaid.
Coverage for weight-management medications varies by carrier and may be available.
Rare Medicaid Exception
A limited exception may exist for secondary cardiovascular prevention.
Typical requirements include:
BMI ≥40
documented atherosclerotic cardiovascular disease
use of a specific Wegovy prior authorization form
Key Takeaways
Determine whether the patient ever had diabetes
Use the correct diagnosis code on the prior authorization
Verify whether the insurance plan covers weight-management medications
Document baseline weight when starting therapy
Consider secondary indications for Medicare coverage
Final Thoughts
Prior authorizations for GLP-1 medications can be complex and time-consuming.
However, many denials occur simply because the submission does not match the insurer’s criteria.
Understanding the differences between diabetes indications, obesity indications, and secondary indications can significantly improve approval rates.
Insurance policies change frequently and vary by plan. This guide reflects common patterns seen in New York, but may not apply to all insurers.
If you found this guide helpful, feel free to share it with colleagues who manage GLP-1 prior authorizations.
I also run a virtual obesity medicine practice focused on complex weight management and cardiometabolic care. If you have patients who would benefit from specialized obesity medicine support, you are welcome to refer them.